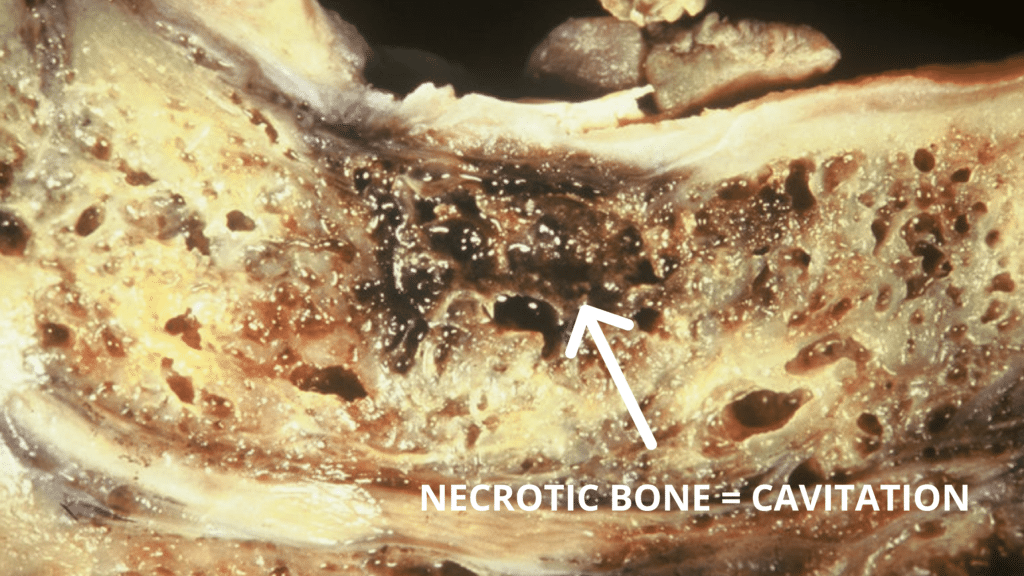
The term, “cavitations,” is a relatively new one in the dental dialogue. Most patients have not heard of cavitations, and most dentists probably do not yet know much about them.
Cavitation can form in any bone in the body, not just in the jawbones. There are other reasons for the formation of cavitations. These reasons may include, among others, localized traumas, poor circulation to the area, clotting disorders, the use of steroids, and, for whatever reason, the individual’s ability to heal properly.
The membrane left behind after the extraction of a tooth can form an image that appears to be a shadow of a tooth when an X-ray is taken of that site. This image may indicate cavitation. Most dentists are aware of this phantom tooth image, but they do not recognize it as a site of potential problems.
Diagnosing cavitations is an elusive process because cavitations do not always readily appear on X-rays. Sometimes they show up only as very subtle differentiations in the texture pattern of the bone. If your dentist is not specifically looking for the cavitations, then your X-ray will be read as looking “just fine.”
There are other ways to discover cavitation sites. For example, when the area with suspected cavitation is lightly stroked or when pressure is applied the patient will sometimes feel pain. I find the EAV instrument is exceptionally useful in helping find cavitation sites; however, it is not recognized as a diagnostic device. The patient must assimilate all the available evidence and decide how he or she wants to proceed with treatment.
Unfortunately, I have seen many patients who have had several cavitation surgeries with no success. The reason the cavitation formed in the first place is still present and unless this is addressed surgery will again fail. I find that by treating the patient on both the physical and nonphysical levels to decrease their toxic load and build up their constitution often cavitations will heal without surgery. For those cavitations that do not spontaneously heal, serval injections of ozone gas directly into the cavitation will usually heal the area. Ozone kills bacteria, viruses, and yeast that are present. Cavitations branch out like tunnels from the main area of infection, and a big advantage of using ozone gas is that the gas follows the infection! In the small percentage of cases that do not respond with the above treatments, surgery can now proceed with a successful outcome.
Specialists have recognized cavitations as a possible cause of chronic facial pain and termed them “NICO” (Neuralgia-Inducing Cavitational Osteonecrosis). Often this is the overlooked factor in trigeminal neuralgia, as well as other kinds of facial pain.
While it is good that the impact of cavitations on facial pain is finally being considered, the far-reaching bodily impact of cavitations is still vastly underappreciated. Cavitations on major meridians can cause serious health problems. I prefer to call cavitations “SICO,” or Sickness Inducing Cavitational Osteonecrosis, which better indicates the power cavitation can have over the general health of the patient. Analysis of cavitational samples by researchers at the University of Kentucky has thus far found every one of them to contain biologically toxic material.
Learn More:
Whole-Body Dentistry by Mark A. Breiner, DDS. Chapter 19 Cavitations
"*" indicates required fields